
Covid-19 is emphatically not the great leveller.
It has shone a light on the great divides in our society. Everyone can catch it, everyone can die from it but the impact of the virus and the necessary measures to control its spread is not shared equally across society.
Our response will require kindness, caring and compassion. The current upsurge in these values should give us cause for hope during an otherwise very difficult time for many people. And they will be most needed where suffering is greatest.
What is interesting about the risk of death or hospital admission from the virus is that it almost perfectly tracks your current risk of death. So, if you are already sick, from a BAME background, grew up in poverty or already older you are more likely to develop serious symptoms and/or die.
The economic impacts will be most acutely felt by those with the fewest resources: people in low paid jobs, people who have chronic mental or physical illness, people on temporary or “zero hours” contracts and those who are living from pay check to pay check. It is also likely that those in low paid manual jobs (e.g. supermarket, social care, construction workers etc) will be less able to socially distance by working from home and, hence, less able to minimise the risk of Covid-19 infection. Those who are now confined to home in poor quality or cramped housing will have the most miserable experience and those living in the least affluent, vibrant and green surroundings will suffer the biggest fall in wellbeing.
These individuals are all part of the same group: the poorest in society.
Michael Marmot recently reminded us that, in the UK, the poorest 10% of households have less than 30% of their income remaining after deducting housing costs and the cost of healthy food. They also have very little wealth to fall back on in times of economic crisis. The implications are clear: loss of income due to Covid-19-related unemployment or illness will cause destitution among those who are already struggling to get by.
Health inequalities were already widening before Covid and these divides are now likely to be accelerated by another economic crisis, massively compounded by a virus that kills those already suffering from chronic illness and multimorbidity, the rates of which already follow a sharp social gradient.
Covid has taken the social determinants of health, which have insidiously been working away behind the scenes, slowly eroding peoples’ health and wellbeing, and exploded their impact into full view. Our civic, community and healthcare resources have been degraded by a decade of austerity, as have many aspects of the welfare safety net. Covid has triggered substantial reinvestment but we must not let these issues disappear back into the shadows as the crisis recedes.
The response to Covid has been to put the whole NHS on an acute footing, aimed at treating a single disease, whilst trying to also provide care to the non-Covid acutely unwell. This means that planned primary care, which can narrow the health gap by 10-20% if access is good and quality high, has been temporarily suspended (or at least deprioritised). Because the system was already at capacity, and because capacity was already inadequate in the most socioeconomically deprived communities, it will take a long time to catch up after this crisis. After Covid we will discover a massive pool of morbidity, mortality and unmet demand. Mental illness that existed before this crisis will also sharply deteriorate due to increased stress and isolation plus a temporary withdrawal of face to face primary care.
GPs also know that the aftermath of social trauma can last years or even decades and blight peoples’ whole lives. GPs have spent years trying to help people traumatised by war, tragic events, childhood neglect or mistreatment, crime or domestic abuse. Covid will leave thousands, perhaps hundreds of thousands, of people traumatised by its direct effects or as a result of vulnerable people being left isolated in toxic social situations, where the abuse or mistreatment they have suffered becomes temporarily inescapable.
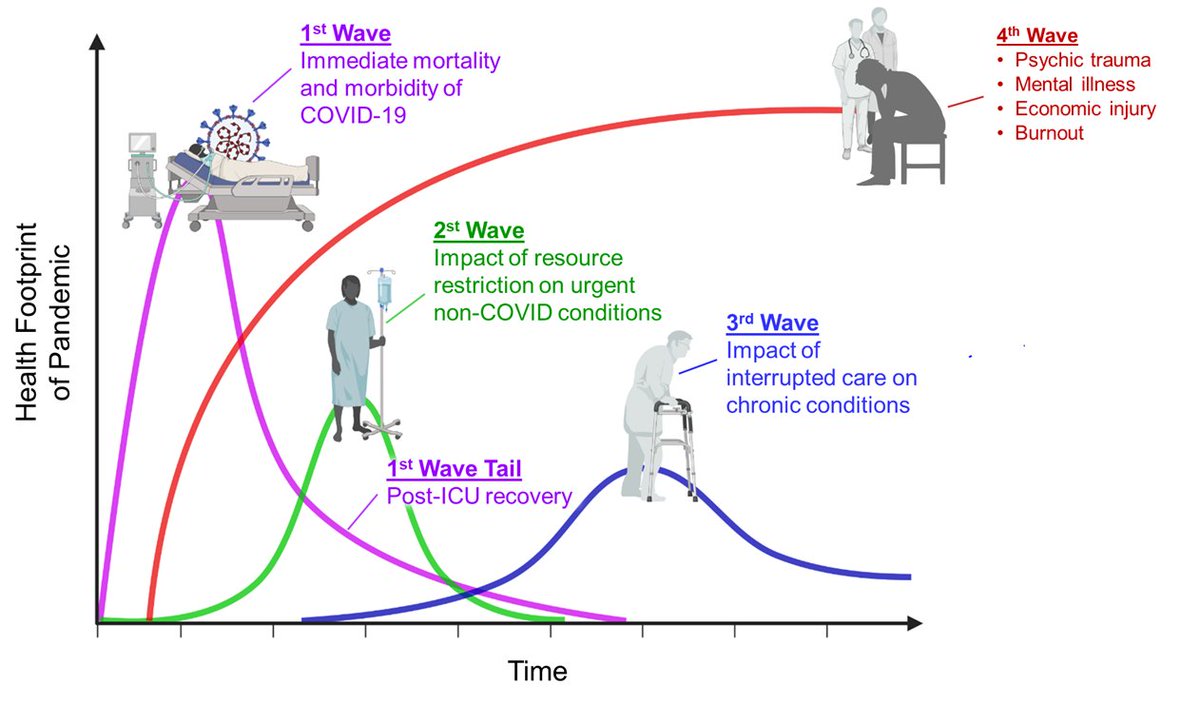
The long tail of this crisis are neatly summarised here:

Source: https://pbs.twimg.com/media/EUX2TipWoAMa_19.jpg (thank you to Dr Victor Tseng)
{kind=link}
So how can we respond?
If there is a positive thing to take away from the Covid crisis it is the outpouring of kindness, the renewed recognition of the contribution of people with jobs whose value may have been forgotten or overlooked, a huge injection of investment into healthcare and social welfare and a revived willingness to think about the needs of others.
We might reflect on J.B. Priestley’s words:
“We don’t live alone. We are members of one body. We are responsible for each other.”
An Inspector Calls, 1945
So how should we respond in primary care?
As our colleagues at Citadel Healthcare in Greater Manchester remind us, for general practice, we should go back to basics: “find the sickest, and give them the best care”. And we must double down on our efforts to do this during and after Covid-19.
- We will have to catch up peoples’ chronic disease management – prioritise the poorest, who can be identified by integrating the available databases on socioeconomic deprivation with primary care records and by examining chronic disease data (time to collaborate with our wonderful colleagues in public health – at Fair Health we are also trying to create some resources to make this easier for practices, watch this space!). Also prioritise those things that have the biggest impact on health outcomes – start with cardiovascular disease prevention. Perhaps revise where to focus your efforts by working through our learning modules.
- Now will be the time to adopt an approach based on “Trauma Informed Care”. You can read more about this in our learning modules on this site and on the “A Better NHS” blog (see resources below).
- Use the Primary Care Network DES to invest in social prescribing to try and deal with some of the acute social issues that Covid will exacerbate and use this to build better links with your local Voluntary and Charitable Sector, who may need your support and advocacy more than ever
- Collaborate with the “social determinants of health workforce” more than ever:
- The social workers, teachers, school nurses and health visitors who will be helping safeguarded children during and after the crisis
- The Citizens Advice Bureau, debt advisors and Department for Work and Pensions operatives who will be needed more than ever to help people through the multiple domestic financial crisis that Covid will create
- Organisations providing care for people who are homeless, refugees and other vulnerable groups to ensure they can access very strained services in the post Covid world
- Drug and alcohol services, whose users won’t have been able to socially distance and access support as easily during this crisis
- The nurses and carers out in the community supporting our most vulnerable
- Remember that primary care organisations are anchor institutions for many communities – just being there is so important: you can hold onto the memories of how Covid impacted your community and you can hold the NHS leadership and politicians to account for their decisions, their efforts to address health inequalities and future readiness for a pandemic or the slower health “emergency” represented by growing health inequalities
- Try and ensure that information about Covid and the social safety net that is being created is accessible to all by providing information in multiple languages and formats (see resources for free translations of material provided by Doctors of the World)
- As illustrated above, the Covid crisis will have a long tail, perhaps stretching out over many years, this is where health equity focussed primary care will be needed most
Resources
A Better NHS Blog: https://abetternhs.net/ (see 23rd February 2020)
The Marmot Review 10 Years On: https://www.health.org.uk/publications/reports/the-marmot-review-10-years-on
Doctors of the World patient information: https://www.doctorsoftheworld.org.uk/coronavirus-information/
Please note that we cannot verify the accuracy of information on external sites, particularly at this time of rapidly changing knowledge about Covid-19